|
Gout is a common metabolic disease predominantly affecting middle-aged individuals and primarily involving peripheral joints. It may occasionally affect the axial skeleton, including the SIJ and sometimes with symptoms mimicking axSpA, doi:10.3899/JRHEUM.080374.
The SIJ appearance by MRI is not specific being characterized by the occurrence of bony erosions filled with a material of intermediate-to-low signal intensity on T1-weighted sequences as well as on STIR/T2FS (Figure 23) usually with accompanying BME and intraarticular joint fluid. CT, especially dual energy CT (doi:10.5152/EURJRHEUM.2019.18097) may assist in the diagnosis by displaying well-defined erosions and sometimes intraarticular mineralization.
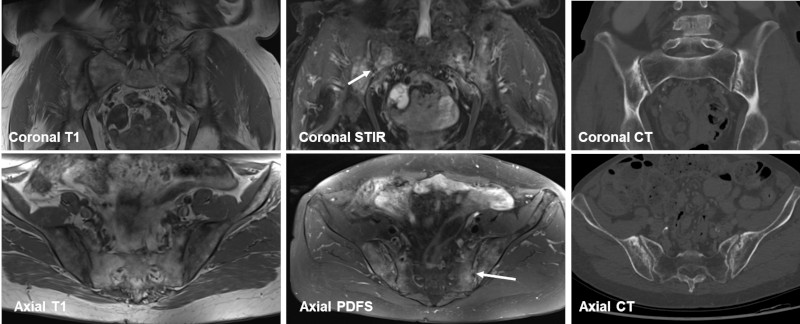
MRI and CT in a patient with low back pain and confirmed crystal deposition in the SIJ. Straight coronal and axial T1, coronal STIR and axial proton fat suppressed (PDFS) images in addition to CT reconstructions in the same planes. There are relative well-defined erosions filled with a material of intermediate-to-low signal intensity on the T1 image with dispersed surrounding sclerosis and small fat depositions. The STIR and PDFS images show inhomogeneous edema in the joint space with intraarticular small signal void areas (arrows) and there is surrounding pronounced BME involving both the sacrum and the ileum. The well-defined erosions are more clearly delineated on the CT images. |