|
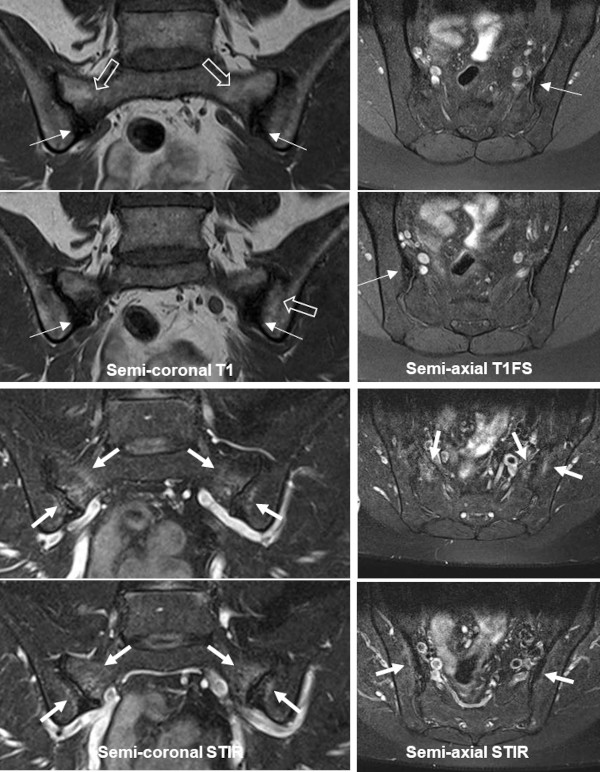
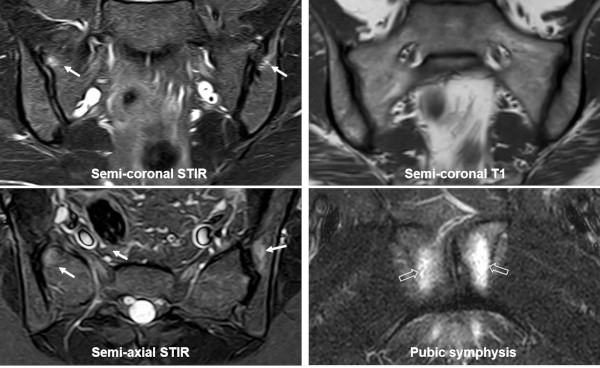
OCI is originally defined based on its radiographic appearance with unilateral or bilateral triangular-shaped sclerosis in the ileum corresponding to the weight-bearing portion of the SIJ, spared SI joint space and no evidence of erosions. OCI can be an asymptomatic incidental finding, but can also present with low back or SIJ pain. It occurs predominantly in females, especially postpartum women, but is occasionally diagnosed in men and nulliparous women where it is often related to obesity or excessive physical load to the SIJ.
Characteristically there are normal inflammatory biomarkers and HLA B27 negativity.
The pathophysiology of OCI is not fully elucidated, but previous pregnancy-related strain to the SIJ often seems to play a role, probably combined with hormonal changes. |