When possible, it is important to diagnose fractures before they are dislocated and potentially giving rise to neurological deficits. Hence the following guidelines.
The possibility of spinal fracture must always be considered when an AS patient reports:
- A direct or indirect spinal trauma, even minor trauma.
- Newly onset of mechanical back pain that is triggered or worsened by activity and completely or partially relieved by rest.
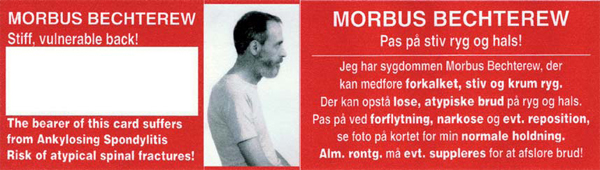
- Changes in posture; if necessary, check photo of the patient on the information card.
- Occurrence of new neurological symptoms (even weak). These can occur immediately after a trauma or be delayed for hours or days.
When substantive suspicion of fracture is present, the following is important:
- Manage the patient as having an unstable fracture until the diagnosis is excluded.
- Avoid the use of rigid cervical collar, if it does not immediately fit the patient's shape.
- Do not attempt to correct a kyphotic spine.
- When positioning and moving the patient, support the entire spine in the position present before the trauma.
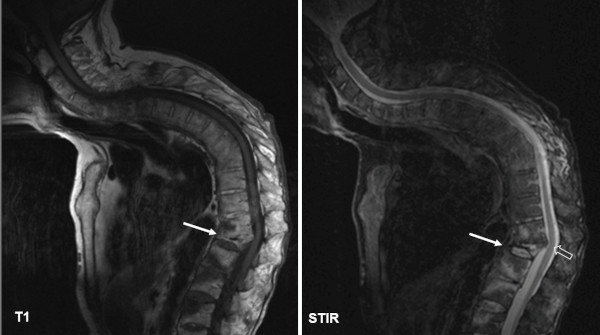
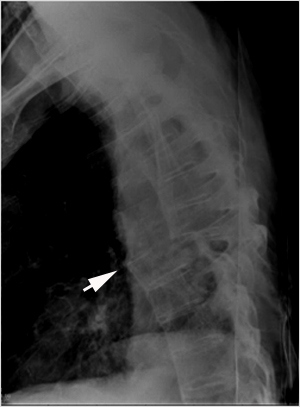
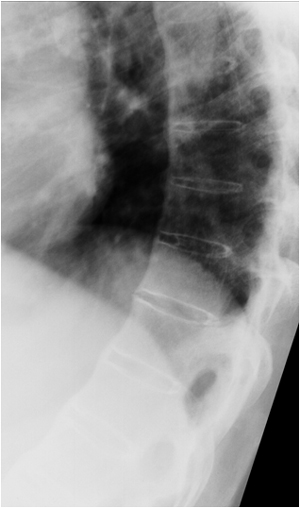
Diagnostic Imaging:
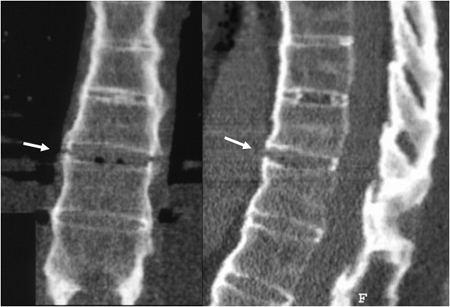
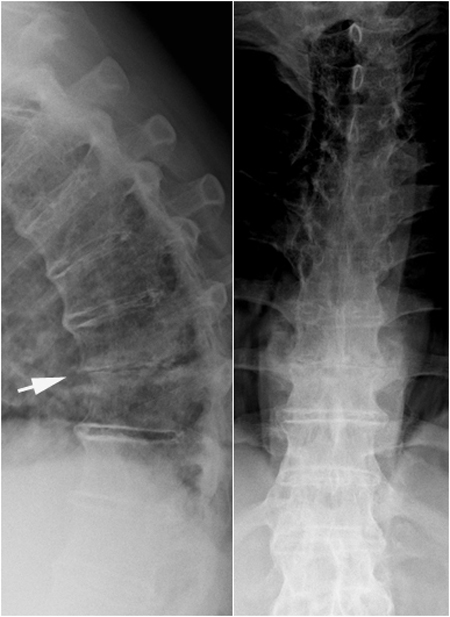
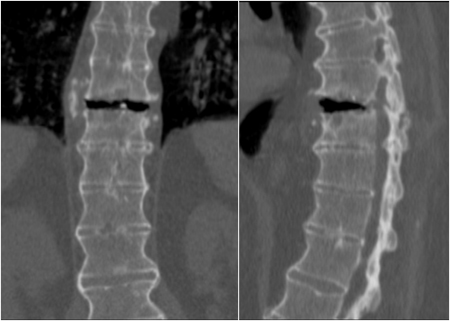
Conventional radiography in at least two planes is often the initial examination. It can be used to diagnose osteoporotic compression fractures and show obvious transverse fractures.
|